We’ve all seen headlines proclaiming that certain foods cause cancer – in fact, the media sometimes make it feel like pretty much everything causes cancer.
But that’s not quite truthful. These headlines are based on a type of research that, although valuable to discover potential links to cancer, can’t prove that something actually causes cancer.

However, scientists often need to know whether one thing causes another. For example, when developing new cancer treatments, we need to know for sure that our new medicine is what cured a patient. So, what can we do? That’s where clinical trials come in.
What are clinical trials?
Trials test medical interventions, which can be things like new medicines, surgeries, changes to treatment protocols, or activities like physiotherapy. They are the culmination of years of research and can only happen when there is significant evidence of an intervention’s safety and potential success. Because trials can test so many types of interventions, we’ll stick to treatments in this blog to avoid confusion.
Clinical trials are a structured way of finding out whether a treatment has the desired effect, for example whether it can improve survival or reduce side effects.
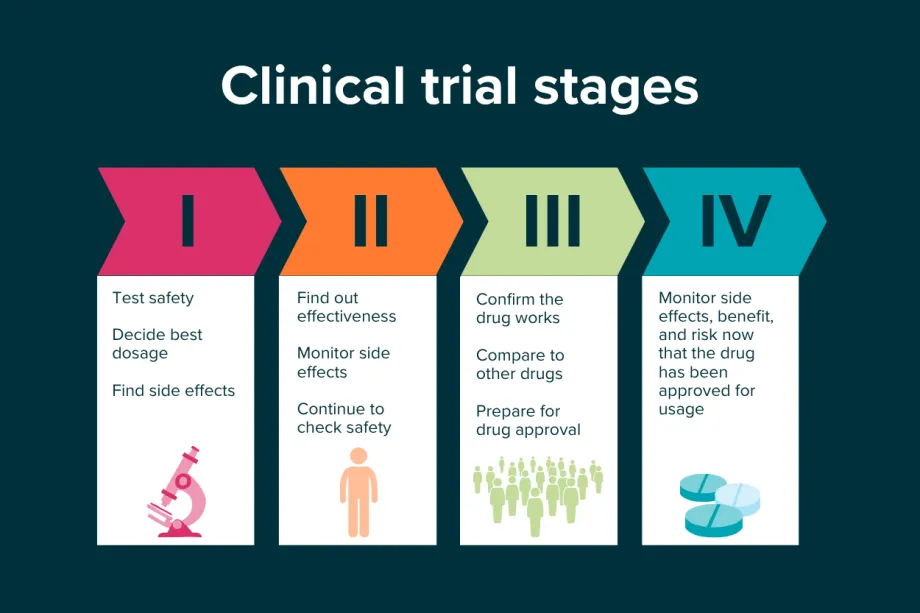
Traditionally, clinical trials have four phases. The first phase uses a small group of patients to help show what the best dose of a medication is, or the best method of delivering it, and make sure that it is safe. Human bodies are complicated, so sometimes treatments that worked in the lab can cause unexpected side effects.
Phase II tests whether the medicine is effective and gathers longer-term safety data. Phase III is where the researchers test if their treatment is better than the current options, using much larger groups of patients. Both phases can include control groups, which are a key part of trials. These patients receive the current standard treatment, so researchers can fairly compare whether a new treatment is actually better. Without this, it would be hard to know what’s really making the difference.
Often, patients are randomly assigned to have either the new treatment or to a control group. This ensures that bias doesn’t affect the results. For example, if a doctor chooses to only give their most ill patients the new treatment, the treatment might look like it doesn’t work, just because those patients were too ill to be cured.
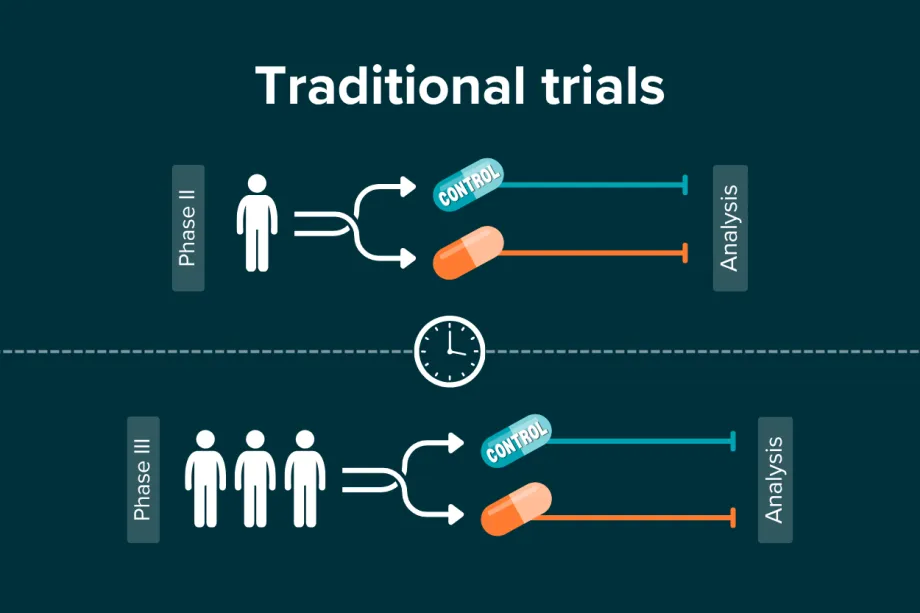
Phase II and Phase III trials usually test new treatments (in orange) against current treatments (in blue). There is often a lot of time between phases, meaning that Phase II participants may not be part of the larger patient group in Phase III.
If Phase III is successful, the treatment will be approved. However, that’s not the end of the clinical trial process - the final phase monitors patients to make sure there are no long-term side effects or problems.
Trials and tribulations
Traditional four-phase clinical trials are effective, but can be slow, expensive, and need large groups of patients. There are also questions about whether it is fair to randomly choose who gets a new, potentially life-saving treatment when multiple patient groups could benefit.
Our understanding of cancer has also made it more difficult to get the large numbers of patients needed for these trials. Cancer types can be broken down into subtypes, subtypes into smaller subgroups, and these groups even further by different genetic mutations – which researchers are still discovering. Now that we understand the importance of subtypes and mutations, a large group of patients with one cancer is fractured into many smaller groups, all of whom may respond differently to treatments. This is one of the reasons that many clinical trials now recruit patients internationally.
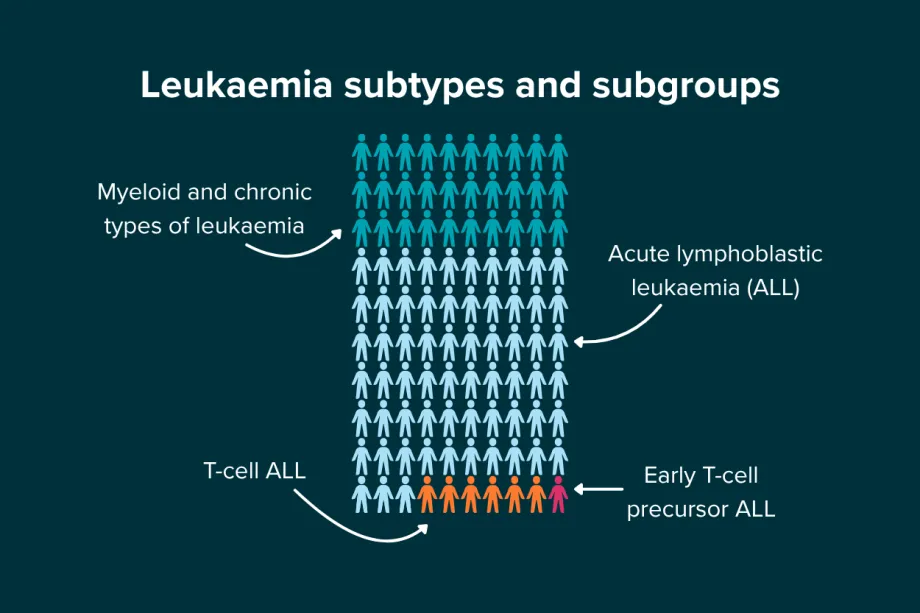
Each year, 450 children are diagnosed with leukaemia. If researchers want to work on just one subgroup, like early T-cell precursor ALL, there are only around 60 patients with that cancer - and that’s not even the rarest type.
Adapting trials
So, what can we do? To speed up improvements for patients, even in children and young people’s cancers where very few patients are diagnosed each year, researchers have developed a number of innovative new clinical trial designs.
Many of these designs are adaptive – which means that researchers can plan in contingencies to respond to early data. For example, if a medicine wasn’t showing any success, their plan might say to drop it from the trial or replace it with another. These trials are often also multi-arm, meaning that they test multiple new treatments at once, so that treatments can be assessed more quickly and efficiently. A benefit of multi-arm trials is that they can often share a control group, instead of each treatment needing its own control group.
Some designs have also moved away from randomly assigning patients to different groups – instead doing complex statistics to find out which treatment has the most potential for success each time a patient joins the trial, assigning them to the arm that is the most promising.
So, let’s look at some of the innovative clinical trial designs that childhood cancer researchers are already using in trials like ESMART and ALLtogether-1.
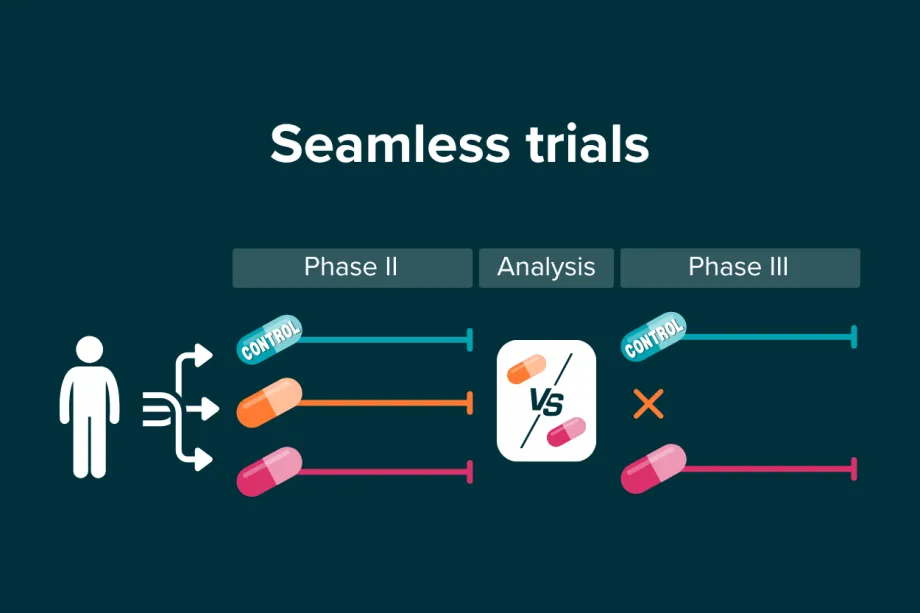
Seamless clinical trials include multiple phases (usually I and II, or II and III) but analyse the data between phases. It can be quicker, as the researchers don’t need to plan or get funding for two completely separate trials. Instead of the first phase ending and then there being long waits and more complicated set up, seamless trials can continue on if their early results show that the treatments are worth continuing. They can also adapt - if their analysis showed that one new treatment was better than the other, the second could be stopped. This ensures children don’t continue along ineffective treatment arms, and saves resources.
This design is useful for childhood cancer because it can reduce the number of patients needed overall – instead of recruiting for two separate studies, the same patients seamlessly continue on the treatment. It can also give the researchers more information about the safety of the treatment longer-term.

From top left: CCLG's Big Hike fundraising walk, Jamie's paddleboard challenge for #PearlPower, Just George's golden ball, Ethan's blindfolded hike, Mini Athletics special classes, and John's six half marathons.
Basket trials ask if a treatment can cure multiple different cancers, instead of asking if it can cure one cancer. Rather than separating out tumour types and each cancer having its own clinical trial, basket trials look for common elements across multiple different cancers. For example, research shows that many childhood cancers are driven by a genetic mutation called MYCN. A basket trial may test one or more treatments that combat MYCN for any patients with that mutation, regardless of cancer type. This naturally means that there is a much larger group of patients enrolled.
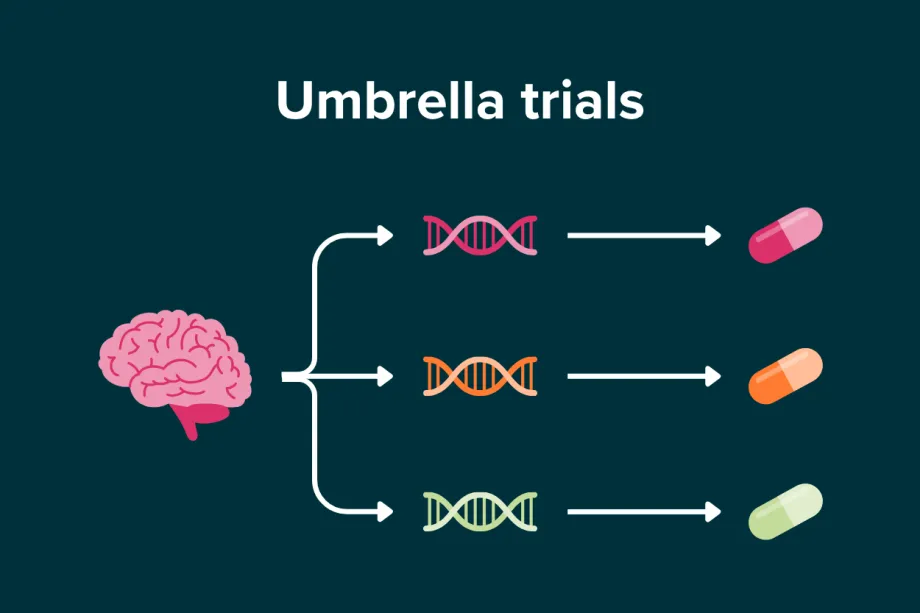
Umbrella trials are the opposite approach to basket trials – they study one cancer, but in lots of detail. Each subtype of the cancer, for example splitting up brain tumours based on genetic mutations, is given a different treatment. Outcomes like survival are compared to standard treatment outcomes. This shows whether the subtypes do need their own targeted treatment approach, rather than using existing one-size-fits-all type treatments.
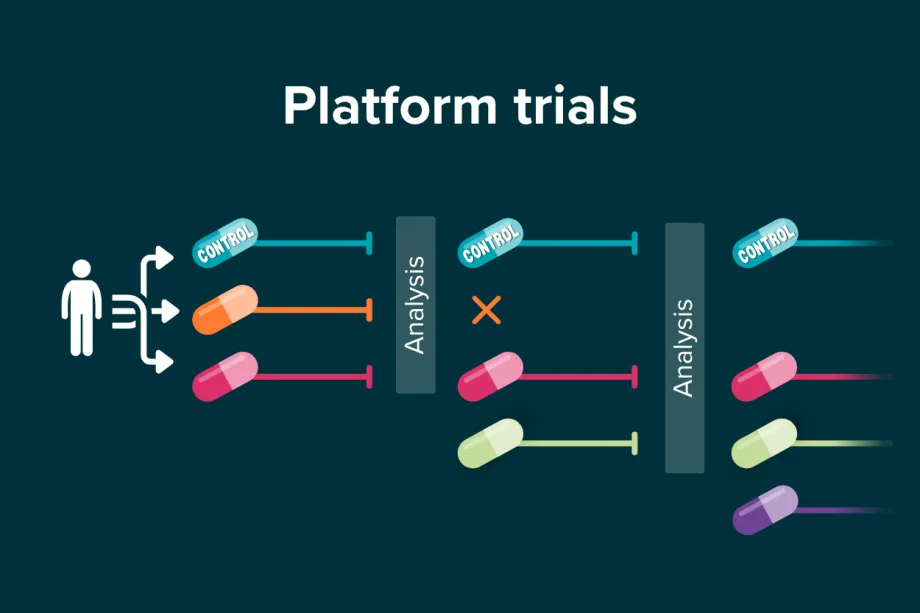
Platform trials are like multi-arm studies, in that they test multiple treatment options, but what makes them different is how adaptive they are. Rather than all of the arms being set when the trial starts, new treatments can be added in later, allowing the trial to stay up to date and include the very latest research. Platform trials can be seamless, with set times planned in for analysis, where ineffective treatments can be removed and new ones added in.
This adaptivity allows them to run much longer than normal trials. Platform trials can stay active for years - the longest running one, in prostate cancer, has been going since 2005. This means that they can collect a lot of data, which is immensely valuable for continued research.
So, there you go – a whirlwind tour of clinical trials and how researchers are adapting to both the challenges of researching rarer cancers and the pressing need for improvements as soon as possible. Most of these modern trial designs more like a group of sub-trials than one trial alone. The sub-trials all benefit from the infrastructure, such as trained personnel and established data collection methods, making research into small groups of patients much more feasible. There’s lots of exciting combinations of these trials, and even more designs are in the works – such as trials where treatments are offered at home or personalised on a patient-by-patient basis.
The main takeaway is that researchers know that families need answers now, and that the traditional trials are not always the right way to achieve that. They are working incredibly hard to make sure that every child and young person gets the very best care possible, whether as part of a clinical trial now, or into the future.
Our Taking Part in Clinical Trials booklet is designed for parents and carers of children and young people with cancer, to help understand more about clinical trials and answer some of the questions they may have.
We'd love to hear what you thought about this blog - please share your feedback here!

Ellie Ellicott is CCLG’s Research Communication Executive.
She is using her lifelong fascination with science to share the world of childhood cancer research with CCLG’s fantastic supporters. You can find Ellie on X: @EllieW_CCLG


