There are two forms of retinoblastoma:
- heritable form – passed on in the family and some children have an affected parent: tumours are often in both eyes (bilateral) or sometimes only in one eye
- non-heritable form - this is not passed on in the family and only one eye is affected
Causes of retinoblastoma
In nearly all cases, retinoblastoma is caused by an abnormality in the retinoblastoma gene (RB1). In the heritable form of retinoblastoma, which accounts for around half of all cases, this abnormal gene is either inherited from a parent or happens for the first time at an early stage of development in the womb.
Genetic counselling and support is available for families in which a member has retinoblastoma. Not all children of a parent with retinoblastoma will inherit this gene, but children born into families with a history of retinoblastoma are offered blood testing to look for the abnormal gene. Children found to have inherited the altered RB1 gene from a parent or those known to be at risk will be offered screening. Screening usually starts shortly after birth and is repeated regularly. This means that treatment can be started early if a tumour does develop.
In the non-heritable form of retinoblastoma, the abnormality in the RB1 gene occurs in just one cell on the retina. The reason for this happening is unknown.
Signs and symptoms
In some children with a family history of retinoblastoma, a tumour is picked up by screening before they have any symptoms.
If there’s no family history of retinoblastoma, the first sign of the condition is often a white pupil that does not reflect light (leucocoria). This may be picked up when a picture of your child is taken using a flash. The pupil of the affected eye may look white in the photograph (see below).
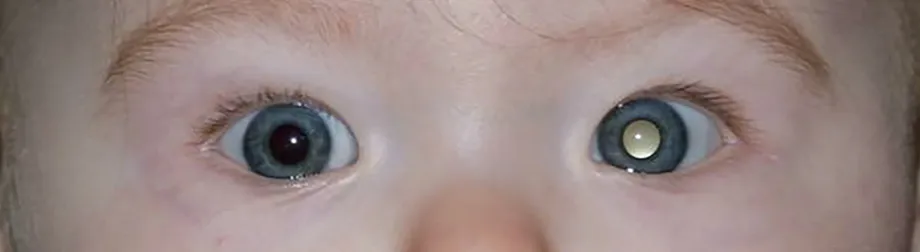
Kindly reproduced with permission from the Childhood Eye Cancer Trust (CHECT)
Some children may have a squint or, if the tumour is large, they may have a painful eye.
Read the Childhood Cancer Eye Trust's symptom checklist for more information
How a retinoblastoma is diagnosed
A variety of tests and investigations may be needed to diagnose retinoblastoma. Any tests and investigations that your child needs will be explained to you. If the doctors suspect that your child may have retinoblastoma, you will be referred to one of the two specialist centres in the UK for confirmation of the diagnosis and treatment. These centres are in Birmingham and London.
Examination under anaesthetic (EUA) – a specialist (ophthalmologist) examines your child’s eye while they’re asleep. Retinoblastomas can be diagnosed by their appearance. Your child will have more EUAs during and after treatment.
Your child may have other tests to check the size and position of the tumour, and whether it has spread into surrounding structures. These tests may include:
- ultrasound scan
- lumbar puncture (spinal fluid sample)
- bone marrow sample
- blood test
- MRI scan
- OCT (optical coherence tomography) scan - uses reflected light to create detailed images of the back of the eye
- AFS (aqueous fluid sampling) - obtains DNA from the tumour by taking a small amount of fluid from the front of the eye; this helps doctors understand more about the genetics of the tumour
Staging
The stage of a cancer is a term used to describe its size and whether it has spread from where it first started. Knowing the type and stage of your child’s retinoblastoma helps the doctors to decide on the most appropriate treatment.
The following staging system is commonly used for retinoblastoma:
Intraocular retinoblastoma
There is cancer in one or both eyes, but it has not spread to the tissues surrounding the eye. This stage may be sub-divided into five grades, depending on the size and position of the cancer and on whether there’s any damage to the eye. The two most commonly used staging systems are IIRC (staging from A to E) and TNM system (staging from cT1 to cT4).
Extraocular retinoblastoma
The cancer has spread outside the eye into the nerve, surrounding tissue, or to other parts of the body.
Treatment
Treatment will depend on the number, position, and size of tumours in your child’s eye. The aim of treatment is, firstly, to get rid of the cancer and, secondly, to try to keep as much sight as possible. Your child’s doctor will talk to you about the possible risks as well as the advantages of the treatment your child is offered.
Local therapy
For smaller tumours, treatment can be given to the eye while your child is asleep under anaesthetic. This is called local therapy and any combination of the following methods may be used:
Cryotherapy
This is a freezing treatment applied to the outside of the eye. More than one session may be necessary, in which case they are usually done at monthly intervals.
Laser therapy
A laser is directed through the pupil and used to heat the tumour. Your child may need a number of sessions of laser therapy (under general anaesthetic) at intervals of 3-4 weeks.
Plaque
A small radioactive disc is stitched on the outside part of the eye overlying the tumour. This disc needs to stay in place for up to four days while the radiation destroys the cancer cells. During this time your child will need to stay in hospital in isolation. This method is used for slightly larger tumours, or for tumours that have not been successfully treated with other methods.
Thermotherapy
This process uses heat to destroy the cancer cells and may be combined with chemotherapy or radiotherapy, as heat can improve the effectiveness of these treatments. The heat is produced by a laser, which is directed at the tumour.
Chemotherapy
Chemotherapy is the use of anti-cancer drugs to destroy cancer cells and may be used for larger tumours, if the cancer has spread, or if there’s a risk that it may spread. It is usually used in combination with local therapy. The drugs most commonly used to treat retinoblastoma are carboplatin, etoposide, and vincristine. Your child’s doctor will discuss which is most suitable for your child.
- systemic chemotherapy is given into the veins – it may be given before any local therapies, to help shrink the tumour and make treatment more successful
- intra-arterial chemotherapy (IAC) is injected directly into the blood vessel that supplies the eye – it allows higher doses of chemotherapy to reach the eye with less side effects to the rest of the body than systemic chemotherapy; IAC may be used instead of systemic chemotherapy, or when the tumour has not responded to initial treatment
- intra-vitreal chemotherapy (IViC) is injected into the central gelatinous part of the eye – it allows higher doses of chemotherapy to reach this area and is used to treat retinoblastoma seeds or recurrences on the retina, and is usually combined with either systemic chemotherapy or IAC
Surgery
If the tumour is more advanced and the vision in the eye is lost, your child may need an operation to remove the eye. This operation is called an enucleation. The specialist will only do this if it is absolutely necessary. An artificial eye is then fitted.
Proton beam radiotherapy
Radiotherapy uses high energy rays to destroy the cancer cells. Radiotherapy may be used if there are cancer cells left behind in the orbit or optic nerve after enucleation or to treat retinoblastoma in the eye when other treatments have not been successful. It can be given to the whole eye but does have some effect on the surrounding tissue. Radiotherapy for retinoblastoma is normally only used when other treatments have not worked well.
Follow-up care
At least 9 out of every 10 children with retinoblastoma are cured. Once treatment has finished, the doctors will monitor your child closely with regular examinations under anaesthetic to check the retina is healthy, the cancer has not come back, and no new tumours have developed. Your child’s general health and any long-term effects will also be monitored. After a while, you will not need to visit the clinic so often. Children with heritable retinoblastoma will be given genetic counselling when they are old enough to understand it.
Having the heritable form of retinoblastoma can mean an increased risk of developing other types of cancer later in life. Your child will be followed up closely into adulthood. They will be encouraged to get any new symptoms, such as a lump, checked early, and to have a healthy lifestyle to help to reduce cancer risk. This includes:
- Avoid smoking
- Careful skin protection in the sun (SPF30 as a minimum)
- Healthy diet
- Exercise
- Moderate alcohol